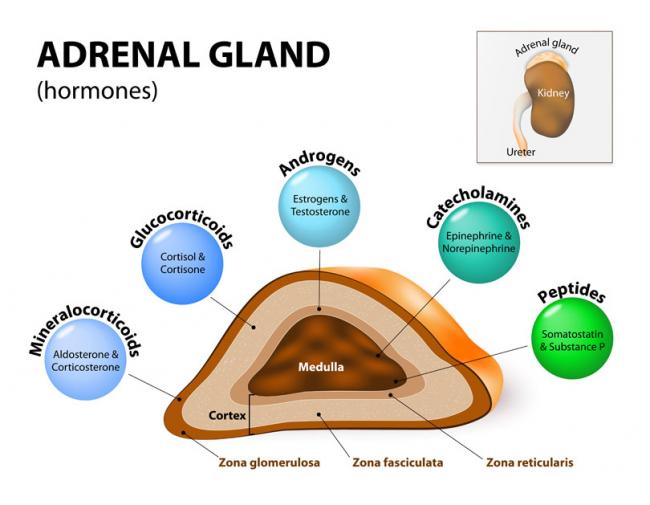
Stressed? In today’s world, we often hear about our adrenal glands being taxed and not performing optimally. Usually, we attribute this to external stressors such as work overload, emotional liabilities, relationship responsibilities, or financial strains. Have you ever thought this could be due to a genetic defect, though?
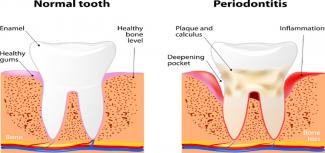
Sure, dental cleaning is great for our oral health, but did you know that it can also improve the wellness of your whole body? Daily toothbrushing and flossing is crucial to maintain the health of our gums and teeth; however, this might actually be more important in pregnant women and those looking to conceive.


OCP is one of the most-used forms of contraception in Canada, but more and more women are looking to alternatives to oral hormonal contraceptive methods.

 The number of couples experiencing infertility and/or resorting to assisted reproductive technology (ART) is on the rise. A study released in 2012 found that among Canadian couples (women aged 18–44 years), the prevalence of infertility ranged from 11 to 15%, and this was an increase compared to previous statistics.
The number of couples experiencing infertility and/or resorting to assisted reproductive technology (ART) is on the rise. A study released in 2012 found that among Canadian couples (women aged 18–44 years), the prevalence of infertility ranged from 11 to 15%, and this was an increase compared to previous statistics. 
 Understanding your menstrual cycle involves more than just estimating your next period. Knowing your body and tracking your menstrual cycles can provide insight into your hormonal and reproductive health. You might be experiencing symptoms that we usually label as “normal,” when we should be calling them “common.”
Understanding your menstrual cycle involves more than just estimating your next period. Knowing your body and tracking your menstrual cycles can provide insight into your hormonal and reproductive health. You might be experiencing symptoms that we usually label as “normal,” when we should be calling them “common.”


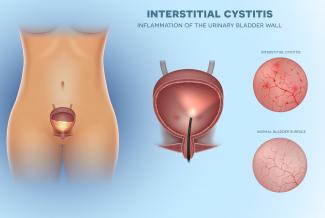
Vaginal infections are a common cause for women to either seek help from their doctor, or to self-medicate with over-the-counter preparations. It’s hard not to self-prescribe with so many easy applications available for yeast infections.

 Vaginal yeast infections can be extremely uncomfortable and significantly impact the quality of a woman’s life. At least 75% of women will experience a yeast infection once in their lifetime, with 45% experiencing two or more episodes, and 5–8% experiencing frequently recurring infections over the course of their life.
Vaginal yeast infections can be extremely uncomfortable and significantly impact the quality of a woman’s life. At least 75% of women will experience a yeast infection once in their lifetime, with 45% experiencing two or more episodes, and 5–8% experiencing frequently recurring infections over the course of their life.

 Whether by unmediated naturals means, induction, or caesarean section, the birth of a child can be an exciting, frightening, and overwhelming experience, and all this is just within in the first moments of life! While some birth experiences go on exactly as planned, others are not as routine, and fortunately procedures such as caesarean delivery (CD) are available to those who might otherwise suffer the negative consequences that can be associated with the birthing process.
Whether by unmediated naturals means, induction, or caesarean section, the birth of a child can be an exciting, frightening, and overwhelming experience, and all this is just within in the first moments of life! While some birth experiences go on exactly as planned, others are not as routine, and fortunately procedures such as caesarean delivery (CD) are available to those who might otherwise suffer the negative consequences that can be associated with the birthing process.

 Who we are and how we feel is often expressed through our hair. Regardless of if hair is curly, straight, twisted, corn-rowed or locked; it is a universal sign of beauty, sensuality, fertility and attractiveness. Moreover, hair helps us to communicate our state of health. It also serves the function of protecting our heads and skin, adding not only a layer of insulation, but also more dimension to our personalities.
Who we are and how we feel is often expressed through our hair. Regardless of if hair is curly, straight, twisted, corn-rowed or locked; it is a universal sign of beauty, sensuality, fertility and attractiveness. Moreover, hair helps us to communicate our state of health. It also serves the function of protecting our heads and skin, adding not only a layer of insulation, but also more dimension to our personalities.

Your period is late—really late. You’re not pregnant, and you’re not menopausal. You may have missed one cycle or several. Of course, it’s worrisome: Many women who have missed one or more periods often take several pregnancy tests just to be certain. But the causes of a missed period go well beyond the possibility of pregnancy.

 Zingiber officinale, known commonly as ginger, has been widely recognized for its action as an antinausea remedy. However, traditional Chinese medicine has used ginger as an anti-inflammatory agent for musculoskeletal complaints for more than 2500 years.
Zingiber officinale, known commonly as ginger, has been widely recognized for its action as an antinausea remedy. However, traditional Chinese medicine has used ginger as an anti-inflammatory agent for musculoskeletal complaints for more than 2500 years.

Hypothyroidism is one of the most common endocrine disorders worldwide. Hypothyroidism and subclinical hypothyroidism have a prevalence rate of 4–5% and 4–15%, respectively. The prevalence is around three to seven times higher in women than men, and its incidences proportionally increase with age.

 Polycystic ovary syndrome (PCOS) is a condition consisting of ovulatory dysfunction and hyperandrogenism, defined as excess activity of testosterone and related androgen hormones. PCOS affects approximately 10% of women of reproductive age, and is a common cause of infertility. However, women with PCOS often suffer from more subtle disturbances in other hormone axes as well, such as thyroid and adrenal systems.
Polycystic ovary syndrome (PCOS) is a condition consisting of ovulatory dysfunction and hyperandrogenism, defined as excess activity of testosterone and related androgen hormones. PCOS affects approximately 10% of women of reproductive age, and is a common cause of infertility. However, women with PCOS often suffer from more subtle disturbances in other hormone axes as well, such as thyroid and adrenal systems.

 Every woman—if she lives long enough—will experience menopause. For some, the transition is easy and can even be a relief from the troubles of a regular menstrual cycle. For others, the change is extremely challenging as they struggle to manage frequent “hot flashes,” weight gain, and severe depression. Many of the symptoms of menopause can be directly related to the decreased production of sex hormones— specifically estrogen and progesterone.
Every woman—if she lives long enough—will experience menopause. For some, the transition is easy and can even be a relief from the troubles of a regular menstrual cycle. For others, the change is extremely challenging as they struggle to manage frequent “hot flashes,” weight gain, and severe depression. Many of the symptoms of menopause can be directly related to the decreased production of sex hormones— specifically estrogen and progesterone.

 Fibroids affect between 5 and 21% of the population and can present with noncyclical pelvic pain, abdominal bloating, constipation, increased urinary frequency, fatigue, dyspareunia (pain during intercourse), and menorrhagia (very heavy menstrual flow)
Fibroids affect between 5 and 21% of the population and can present with noncyclical pelvic pain, abdominal bloating, constipation, increased urinary frequency, fatigue, dyspareunia (pain during intercourse), and menorrhagia (very heavy menstrual flow)

 Gestational diabetes (GDM) is a diagnosis that describes glucose intolerance with the onset of diabetes during pregnancy in a previously nondiabetic woman. With a prevalence of 8–18% in Canadian pregnancies, screening is recommended after approximately 24 weeks gestation.
Gestational diabetes (GDM) is a diagnosis that describes glucose intolerance with the onset of diabetes during pregnancy in a previously nondiabetic woman. With a prevalence of 8–18% in Canadian pregnancies, screening is recommended after approximately 24 weeks gestation.

 Gestational diabetes mellitus (GDM) is a pregnancy complication defined as impaired blood sugar regulation beginning in pregnancy, and is no longer present after delivery. Although prevalence varies, a recent study by the CDC reports that as many as 9.2% of pregnancies are affected by gestational diabetes.
Gestational diabetes mellitus (GDM) is a pregnancy complication defined as impaired blood sugar regulation beginning in pregnancy, and is no longer present after delivery. Although prevalence varies, a recent study by the CDC reports that as many as 9.2% of pregnancies are affected by gestational diabetes.

 It can be difficult for many women to find and utilize non hormonal options when it comes to fertility. This includes women who want to become pregnant but also those who are looking to avoid pregnancy. With many women and couples having misconceptions regarding the fertile period of a woman’s cycle, it is more advantageous to educate women on their fertile signs for greater chances of either conception or avoidance of conception.[1]
It can be difficult for many women to find and utilize non hormonal options when it comes to fertility. This includes women who want to become pregnant but also those who are looking to avoid pregnancy. With many women and couples having misconceptions regarding the fertile period of a woman’s cycle, it is more advantageous to educate women on their fertile signs for greater chances of either conception or avoidance of conception.[1]
 Pregnancy can be one of the most exciting times in a woman’s life. It can also be one of the most stressful times, especially if the pregnancy is complicated with health issues. There are many common and familiar “side effects” of pregnancy, such as nausea, heartburn, and fatigue. However, there are also more serious conditions that can develop following pregnancy, and the symptoms should not be ignored or brushed aside, as they can potentially be signs of new disease onset, and could greatly affect long-term health.
Pregnancy can be one of the most exciting times in a woman’s life. It can also be one of the most stressful times, especially if the pregnancy is complicated with health issues. There are many common and familiar “side effects” of pregnancy, such as nausea, heartburn, and fatigue. However, there are also more serious conditions that can develop following pregnancy, and the symptoms should not be ignored or brushed aside, as they can potentially be signs of new disease onset, and could greatly affect long-term health.

 Thinking of conceiving? You may have heard about the “100 days”—the time it takes for an egg to mature. For men, it takes about 80 days for sperm to mature. During this time of development and maturation, a woman’s follicles and a man’s sperm are extremely vulnerable to DNA damage from exposure to toxins, systemic or chronic inflammation, and nutrient deficiencies. This means that for many who are ready to or are thinking of conceiving in the not-so-far future, the health of their eggs and sperm can be greatly impacted before they are even released, either during ovulation or ejaculation. This is the window that we need to take advantage of, to increase the health of our eggs and sperm to increase the odds of a viable and healthy egg, and fertilization.
Thinking of conceiving? You may have heard about the “100 days”—the time it takes for an egg to mature. For men, it takes about 80 days for sperm to mature. During this time of development and maturation, a woman’s follicles and a man’s sperm are extremely vulnerable to DNA damage from exposure to toxins, systemic or chronic inflammation, and nutrient deficiencies. This means that for many who are ready to or are thinking of conceiving in the not-so-far future, the health of their eggs and sperm can be greatly impacted before they are even released, either during ovulation or ejaculation. This is the window that we need to take advantage of, to increase the health of our eggs and sperm to increase the odds of a viable and healthy egg, and fertilization.